

Overview
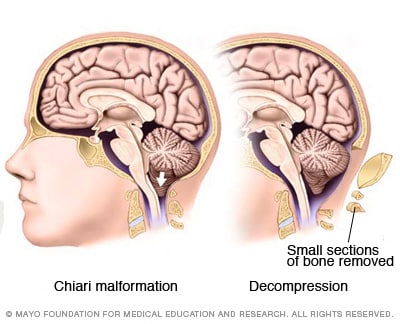
Chiari malformation (kee-AH-ree mal-for-MAY-shun) is a condition in which brain tissue extends into your spinal canal. It occurs when part of your skull is abnormally small or misshapen, pressing on your brain and forcing it downward.
Chiari malformation is uncommon, but increased use of imaging tests has led to more frequent diagnoses.
Doctors categorize Chiari malformation into three types, depending on the anatomy of the brain tissue that is displaced into the spinal canal and whether developmental abnormalities of the brain or spine are present.
Chiari malformation type I develops as the skull and brain are growing. As a result, signs and symptoms may not occur until late childhood or adulthood. The pediatric forms, Chiari malformation type II and type III, are present at birth (congenital).
Treatment of Chiari malformation depends on the form, severity and associated symptoms. Regular monitoring, medications and surgery are treatment options. In some cases, no treatment is needed.
Symptoms
Many people with Chiari malformation have no signs or symptoms and don’t need treatment. Their condition is detected only when tests are performed for unrelated disorders. However, depending on the type and severity, Chiari malformation can cause a number of problems.
The more common types of Chiari malformation are:
- Type I
- Type II
Although these types are less serious than the more rare pediatric form, type III, signs and symptoms still can be life disrupting.
Chiari malformation type I
In Chiari malformation type I, signs and symptoms usually appear during late childhood or adulthood.
Headaches, often severe, are the classic symptom of Chiari malformation. They generally occur after sudden coughing, sneezing or straining. People with Chiari malformation type I can also experience:
- Neck pain
- Unsteady gait (problems with balance)
- Poor hand coordination (fine motor skills)
- Numbness and tingling of the hands and feet
- Dizziness
- Difficulty swallowing, sometimes accompanied by gagging, choking and vomiting
- Speech problems, such as hoarseness
Less often, people with Chiari malformation may experience:
- Ringing or buzzing in the ears (tinnitus)
- Weakness
- Slow heart rhythm
- Curvature of the spine (scoliosis) related to spinal cord impairment
- Abnormal breathing, such as central sleep apnea, which is when a person stops breathing during sleep
Chiari malformation type II
In Chiari malformation type II, a greater amount of tissue extends into the spinal canal compared with Chiari malformation type I.
The signs and symptoms can include those related to a form of spina bifida called myelomeningocele that nearly always accompanies Chiari malformation type II. In myelomeningocele, the backbone and the spinal canal haven’t closed properly before birth.
Signs and symptoms may include:
- Changes in breathing pattern
- Swallowing problems, such as gagging
- Quick downward eye movements
- Weakness in arms
Chiari malformation type II is usually noted with ultrasound during pregnancy. It may also be diagnosed after birth or in early infancy.
Chiari malformation type III
In one of the most severe types of the condition, Chiari malformation type III, a portion of the lower back part of the brain (cerebellum) or the brainstem extends through an abnormal opening in the back of the skull. This form of Chiari malformation is diagnosed at birth or with an ultrasound during pregnancy.
This type of Chiari malformation has a higher mortality rate and may also cause neurological problems.
When to see a doctor
If you or your child has any of the signs and symptoms that may be associated with Chiari malformation, see your doctor for an evaluation.
Because many symptoms of Chiari malformation can also be associated with other disorders, a thorough medical evaluation is important.
Causes
Chiari malformation type I occurs when the section of your skull containing a part of your brain (cerebellum) is too small or is deformed, thus putting pressure on and crowding your brain. The lower part of the cerebellum (tonsils) is displaced into your upper spinal canal.
Chiari malformation type II is nearly always associated with a form of spina bifida called myelomeningocele.
When the cerebellum is pushed into your upper spinal canal, it can interfere with the normal flow of cerebrospinal fluid that protects your brain and spinal cord.
This impaired circulation of cerebrospinal fluid can lead to the blockage of signals transmitted from your brain to your body, or to a buildup of spinal fluid in the brain or spinal cord.
Alternatively, the pressure from the cerebellum on the spinal cord or lower brainstem can cause neurological signs or symptoms.
Risk factors
There’s some evidence that Chiari malformation runs in some families. However, research into a possible hereditary component is still in its early phase.
Complications
In some people, Chiari malformation can become a progressive disorder and lead to serious complications. In others, there may be no associated symptoms, and no intervention is necessary. The complications associated with this condition include:
- Hydrocephalus. An accumulation of excess fluid within your brain (hydrocephalus) may require placement of a flexible tube (shunt) to divert and drain the cerebrospinal fluid to another area of your body.
- Spina bifida. Spina bifida, a condition in which your spinal cord or its covering isn’t fully developed, may occur in Chiari malformation. Part of the spinal cord is exposed, which can cause serious conditions such as paralysis. People with Chiari malformation type II usually have a form of spina bifida called myelomeningocele.
- Syringomyelia. Some people with Chiari malformation also develop a condition called syringomyelia, in which a cavity or cyst (syrinx) forms within the spinal column.
- Tethered cord syndrome. In this condition, your spinal cord attaches to your spine and causes your spinal cord to stretch. This can cause serious nerve and muscle damage in your lower body.
Diagnosis
To diagnose your condition, your doctor will review your medical history and symptoms and conduct a physical examination.
Your doctor will also order imaging tests to diagnose your condition and determine its cause. Tests may include:
- Magnetic resonance imaging (MRI). An MRI is often used to diagnose Chiari malformation. An MRI uses powerful radio waves and magnets to create a detailed view of your body.This safe, painless test produces detailed 3D images of structural abnormalities in your brain that may be contributing to your symptoms. It can also provide images of your cerebellum and determine whether it extends into your spinal canal.An MRI can be repeated over time, and it can be used to monitor the progression of your disorder.
- Computerized tomography (CT) scan. Your doctor may recommend other imaging techniques such as a CT scan.A CT scan uses X-rays to obtain cross-sectional images of your body. A CT scan can help to reveal brain tumors, brain damage, bone and blood vessel abnormalities, and other conditions.
Treatment
Treatment for Chiari malformation depends on the severity and the characteristics of your condition.
If you have no symptoms, your doctor likely will recommend no treatment other than monitoring with regular examinations and MRIs.
When headaches or other types of pain are the primary symptom, your doctor may recommend pain medication.
Reducing pressure with surgery
Doctors usually treat symptomatic Chiari malformation with surgery. The goal is to stop the progression of changes in the anatomy of your brain and spinal canal, as well as ease or stabilize your symptoms.
When successful, surgery can reduce pressure on your cerebellum and spinal cord, and restore the normal flow of spinal fluid.
In the most common surgery for Chiari malformation, called posterior fossa decompression, your surgeon removes a small section of bone in the back of your skull, relieving pressure by giving your brain more room.
In many cases, the covering of your brain, called the dura mater, may be opened. Also, a patch may be sewn in place to enlarge the covering and provide more room for your brain. This patch may be an artificial material, or it could be tissue harvested from another part of your body.
Your doctor may also remove a small portion of the spinal column to relieve pressure on your spinal cord and allow more space for the spinal cord.
The surgical technique may vary, depending on whether a fluid-filled cavity (syrinx) is present, or if you have fluid in your brain (hydrocephalus). If you have a syrinx or hydrocephalus, you may need a tube (shunt) to drain the excess fluid.
Surgical risks and follow-up
Surgery involves risks, including the possibility of infection, fluid in your brain, cerebrospinal fluid leakage or problems with wound healing. Discuss the pros and cons with your doctor when deciding whether surgery is the most appropriate treatment for you.
The surgery reduces symptoms in most people, but if nerve injury in the spinal canal has already occurred, this procedure won’t reverse the damage.
After the surgery, you’ll need regular follow-up examinations with your doctor, including periodic imaging tests to assess the outcome of surgery and the flow of cerebrospinal fluid.
Preparing for your appointment
You’re likely to start by seeing your family doctor. However, when you call to set up an appointment, you may be referred to a doctor trained in brain and nervous system conditions (neurologist).
Because appointments can be brief, and because there’s often a lot to talk about, it’s a good idea to be well prepared for your appointment. Here’s some information to help you get ready for your appointment, and know what to expect from your doctor.
What you can do
- Be aware of any pre-appointment restrictions. At the time you make the appointment, be sure to ask if there’s anything you need to do in advance.
- Write down any symptoms you’re experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment. For example, even though your primary complaint may be headaches, your doctor will want to know about any changes you may have noticed in your vision, speech or coordination.
- Write down key personal information, including any major stresses and recent life changes.
- Make a list of your key medical information, including other conditions you’re being treated for and the names of the medications that you’re taking.
- Take a family member or friend along, if possible. Sometimes it can be difficult to recall all the information provided to you during an appointment. Someone who accompanies you may remember something that you missed or forgot.
- Write down questions to ask your doctor.
Prepare a list of questions so that you can make the most of your limited time with your doctor. List your questions from most important to least important in case time runs out. For Chiari malformation, some basic questions to ask your doctor include:
- What is likely causing my symptoms or condition?
- Other than the most likely cause, what are possible causes for my symptoms or condition?
- What kinds of tests do I need?
- Do I need treatment?
- If you don’t think I need to be treated now, how will you monitor me for changes in my condition?
- If you recommend surgery, what should I expect from my recovery?
- What is the risk of complications from surgery?
- What is my long-term prognosis after surgery?
- I have other health conditions. How can I best manage them together?
- Are there any restrictions that I need to follow?
- Should I see a specialist? What will that cost, and will my insurance cover seeing a specialist?
- Are there any brochures or other printed material that I can take home with me? What websites do you recommend visiting?
In addition to the questions that you’ve prepared to ask your doctor, don’t hesitate to ask questions during your appointment at any time that you don’t understand something.
What to expect from your doctor
Your doctor is likely to ask you a number of questions. Being ready to answer them may reserve time to go over any points you want to spend more time on. Your doctor may ask:
- When did you first begin experiencing symptoms?
- Have your symptoms been continuous or occasional?
- If you experience head and neck pain, is it made worse by sneezing, coughing or straining?
- How severe is your head and neck pain?
- Have you noticed any change in your coordination, including problems with balance or with hand coordination?
- Do your hands and feet feel numb or do they tingle?
- Have you developed any difficulty swallowing?
- Do you experience episodes of dizziness or faintness? Have you ever passed out?
- Have you developed any problems with your eyes and ears, such as blurred vision or a ringing or buzzing in your ears?
- Have you had problems with bladder control?
- Has anyone ever noticed that you stop breathing during sleep?
- Have you been taking pain relievers or using other approaches to relieve your discomfort? Does anything seem to work?
- Do you have any additional symptoms, such as hearing loss, fatigue, or changes in your bowel habits or appetite?
- Have you been diagnosed with any other health conditions?
- Has anyone in your family been diagnosed with Chiari malformation?
